


A selection of clinical research and expert opinion on the effectiveness of wearing masks to protect against coronavirus.
One of many of my old posts deleted by LinkedIn for spreading "misinformation".

All from spring/summer 2020 (yeah, we’ve known for a very, very long time that masks are useless at best). I think this compendium earned me a suspension. Because, you know, Science™.
Many of the original links are now dead due to censorship but here the ones that survived.
For convenience, a selection of clinical research and expert opinion on the effectiveness of wearing masks to protect against coronavirus...
General conclusion and consensus is that masks are not effective for the prevention of viral spread, neither inward nor outward.
Conversely, evidence suggests masks may be detrimental due to myriad other side effects.
No mention of repurposed old t-shirts in the reference material though so you'll have to infer your own conclusions on that.
11th May 2020

Blaylock: Face Masks Pose Serious Risks To The Healthy
30th June 2020
A phlegmatic appraisal of masks vis-a-vis the coronavirus from Chris von Csefalvay, an epidemiologist specializing in bat-borne viruses.
As states begin to reopen and America tries to recreate normalcy, masks have replaced social distancing as the new moral statement.
Just as adherence to lockdowns was framed by many as a sign of virtue — with some arguing that those who refused to abide by the lockdown orders should forfeit medical care for Covid-related indications — masks have become a face-borne signal of righteousness.
As a virologist, I find this perplexing, considering the limited evidence in favor of masks...
The evidence is hardly strong enough to elevate mask-wearing into the epitome of moral behavior.
Doing so reflects a greater preoccupation with the psychological effect of masks — perhaps as a restoration of control in the face of an unseen and often perplexing enemy with no cure and no prophylaxis — than with their scientific reality.
Americans should demand evidence-based decision-making and policies driven by soundly attested facts, not assumptions or psychological palliatives.
A summary of the 15 measures (18 recommendations) from the WHO of "Non-pharmaceutical public health measures for mitigating the risk and impact of epidemic and pandemic influenza".
Note, most of the recommendations have "low" or "very low" quality of evidence or "none" at all.
Also note that a lot of the measures that are NOT recommended have been adopted by many member states, e.g. contact tracing, quarantine of exposed individuals, entry/exit screening, border closures.
Most importantly, quarantine of unexposed, non-symptomtic individuals (aka lockdown, shelter in place, etc.) doesn't even get a mention, let alone in the "not recommended" category.
Keep following the "science" though...

26th Sept 2020

Mask Facts, Association of American Physicians and Surgeons - Marilyn M. Singleton, M.D., J.D.
26th July 2020

Science Says Healthy People Should NOT Wear Masks, Patricia Neuenschwander, M.S.N., R.N., C.P.N.P.-P.C.
25th July 2020

Does Universal Mask Wearing Decrease or Increase the Spread of COVID-19?
25th July 2020

The Science: Masks Are Neither Effective Nor Safe - Dr. Colleen Huber, NMD
10th June 2020

Norway, one of the covid success poster children (who then admitted lockdowns were a mistake).
Honest and trustworthy, their public health authority on masks:
Given the low prevalence of COVID-19 currently, even if facemasks are assumed to be effective, the difference in infection rates between using facemasks and not using facemasks would be small.
Assuming that 20% of people infectious with SARS-CoV-2 do not have symptoms, and assuming a risk reduction of 40% for wearing [medical] facemasks, 200 000 people would need to wear facemasks to prevent one new infection per week in the current epidemiological situation.
...wearing facemasks to reduce the spread of COVID-19 is not recommended for individuals in the community without respiratory symptoms who are not in near contact with people who are known to be infected.
If use of facemasks by individuals without respiratory symptoms in the community is recommended in specific circumstances, medical masks or quality controlled non-medical masks with a documented filtration effect should be used.
...the community should be given training to ensure correct use and the risks should be explained, especially the risks of a false sense of security and contamination of masks.
26th April 2016
Disposable surgical face masks for preventing surgical wound infection in clean surgery
Useful idiot: well, why do surgeons wear masks then??
Me: facemasks have long been thought to confer protection to the patient from wound infection and contamination from the operating surgeon and other members of the surgical staff.
Overall, however, there is a lack of substantial evidence to support claims that facemasks protect either patient or surgeon from infectious contamination.
In order to advocate the validity of an intervention in medicine, it must satisfy three levels of evidence: efficacy, effectiveness and cost-effectiveness.
In the context of facemask, efficacy is whether masks prevent the propagation of droplets derived from the mouth and nose of the operating staff.
Effectiveness is whether efficacy translates into a significant reduction in surgical site infection morbidity and mortality.
And finally, cost-effectiveness determines whether the cost-to-benefit ratio of this effect would be desirable compared to an alternative course of action.
And you really want to believe that non-surgical, universal mask-wearing in community settings comes close to satisfying even one of those criteria??
‘Venting’ is a phenomenon whereby air leaks at the interface between mask and face which can act to disperse potential contaminants originating from the pharynx. The accumulation of moisture, during prolonged usage, may exacerbate this problem by increasing resistance to air flow through the filter itself. Moisture accumulation is also thought to facilitate the movement of contaminants through the material of the mask itself by capillary action. These bacteria can subsequently be dislodged by movement. Friction at the face/mask interface has also been demonstrated to disperse skin scales which can further contribute towards wound contamination.
All valid reasons to claim exemption from wearing a mask in the UK under STATUTORY INSTRUMENTS 2020 No. 791, PUBLIC HEALTH, ENGLAND, The Health Protection (Coronavirus, Wearing of Face Coverings in a Relevant Place) (England) Regulations 2020 Part 4 (1)(d)
"P removes their face covering to avoid harm or injury, or the risk of harm or injury, to themselves or others."
1st August 2020
Telegraph Letters: What do further lockdowns achieve beyond encouraging more hysteria?

Face masks do not reduce the risk of infection
SIR – If face masks did indeed reduce the risk of infection to surgical patients, as suggested by Malcolm H Wheeler (Letters, July 28), all surgeons would wear them. However, in our practices, we discarded masks more than 20 years ago, after a series of controlled trials showed that using them either had no effect on, or sometimes actually increased, the risk of post-operative infection.
Simply observing that Covid-19 infection rates are lower in some countries where mask use is the norm does not prove cause and effect, which explains why bodies advising ministers were so cautious in recommending face covering. We are told that the present requirement to wear masks in shops is meant to give the public confidence. How insisting on a measure shown to be useless or worse in not dissimilar circumstances will achieve this mystifies us.
John Black FRCS
Malvern, Worcestershire
[FORMER PRESIDENT OF THE ROYAL COLLEGE OF SURGEONS OF ENGLAND]
Antony Narula FRCS
Wargrave, Berkshire
[Senior otorhinolaryngologist and elected member of Royal College of Surgeons Council from 2004 to 2014].
5th August 2020
‘Mask mouth’ is a seriously stinky side effect of wearing masks.

6th August 2020
Europe's Top Health Officials Say Masks Aren't Helpful in Beating COVID-19

In the year 2018 BC (Before Covid), Canadian law ruled against "vaccinate or mask" (VOM) policy - the mandatory wearing of masks by presumed healthy nurses who had not been vaccinated against the flu.
"I find that the Policy was introduced at SAH for the purpose of driving up vaccination rates. I also find that the weight of scientific evidence said to support the VOM Policy on patient safety grounds is insufficient to warrant the imposition of a mask-wearing requirement for up to six months every year.
Absent adequate support for the freestanding patient safety purpose alleged, I conclude that the Policy operates to coerce influenza immunization and, thereby, undermines the collective agreement right of employees to refuse vaccination.
On all of the evidence, and for the reasons canvassed at length in this Award, I conclude that the VOM Policy is unreasonable."
6th Sept 2018
St. Michael’s Hospital v Ontario Nurses’ Association, 2018 CanLII 82519 (ON LA)
10th Dec 2016
Cover up: The lack of evidence for vaccinate or mask policies
12th Sept 2018
'Vaccinate or mask' ruling prompts London hospitals to review policies
12th July 2020
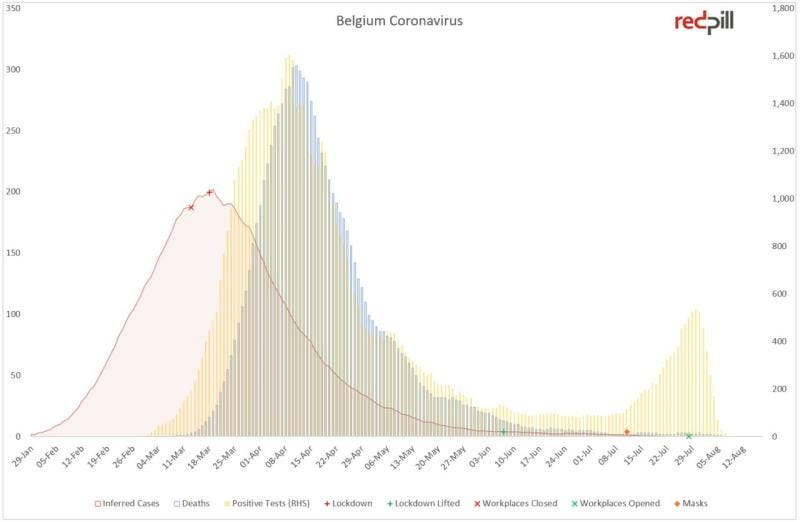
On 11th July, in spite of overwhelming evidence against effectiveness, face masks became mandatory in Belgium for shops and busy commercial outdoor areas. Now, Antwerp, its 2nd largest city is under curfew, and the city of Brussels threatens its inhabitants with mandatory face masks in all outdoor areas.
This only makes sense in 🤡 world where they can't tell the difference between a case and an infection even when you draw them a pretty picture.
Even the untrained eye should be able to detect the pattern of testing people when they were admitted to hospital and the very strong correlation between those tests and deaths, i.e. proper "cases".
Then, around about the 2nd week of July looks like they ramped up community testing and found a whole bunch of asyptomatic "infections", false positives and remnants. Otherwise the rise in infections appears to positively correlate with mandatory masking.
🤔
You probably couldn't get a clearer example of infection-to-death as it happens. 2 - 3 weeks from infection to hospitalisation and 1 week to death. 3 to 4 weeks in total, consistently around the world where HCQ is not administered.
28th July 2020
DR. SHERRI TENPENNY – FACE MASKS ARE NOT EFFECTIVE AGAINST COVID-19: HOW MASKS ARE BEING USED TO CONTROL THE POPULATION
4th August 2020
WHO Admits: No Direct Evidence Masks Prevent Viral Infection
Annals of the Royal College of Surgeons of England (1981) vol. 63 Is a mask necessary in the operating theatre?
I guess you could say I’d done my research, even back then?!
And regardless of who says it, if it doesn’t fit the narrative, it can always be removed…
Thanks Joel. I can't believe we are still talking masks, but useful to have this reference, should they ever try and make a come back.
Here ya go
https://brownstone.org/articles/more-than-150-comparative-studies-and-articles-on-mask-ineffectiveness-and-harms/