


Why are there so many more East German COVID-associated deaths than West German?
Comprehensive analysis of deaths in Germany between 2015 and 2022, by region, age, COVID, and vaccination rates.

Executive Summary
COVID-era deaths in Germany are not distinctly worse than other recent periods.
Unlike prior periods, COVID has been substantially worse for East Germans than West Germans.
Non-pharmaceutical interventions designed for “social distancing” have no impact on mitigation of spread or deaths.
The COVID “vaccine” provides no benefit in reducing transmission or contributing towards herd immunity, casting serious doubts on the scientific validity of vaccine mandates, regardless of the clear ethical concerns.
The COVID “vaccine” makes no difference in reducing COVID deaths.
Relatively more people under 60 died of COVID in the post-vax era than before.
Ultimately, COVID variant selection has resulted in the most transmissible and least virulent, as one would expect to be the natural course of events.
Despite fewer COVID deaths, all-cause mortality remains at the high end of recent levels.
The most likely explanation for higher East German deaths than West German is a combination of poorer health and/or healthcare, and worse climate.
When all is said and done, there is nothing particularly novel about SARS-CoV-2 compared to other seasonal, respiratory pathogens in Germany, except its propensity to kill East Germans rather than West Germans.
Introduction

Looking at deaths of all causes and ages in Germany during the COVID era does not appear to be any more remarkable than before.
In fact, according to Figure 1, when COVID first emerged in spring 2020, Germany’s death tally was more-or-less identical to the previous season, which in turn was a relatively low one.
When COVID did hit the following autumn/winter, it is still not so remarkable, registering not dissimilar numbers to the 2017-18 season, taking into account an already rising baseline.
The most recent season (2021-22) is not discernibly smaller in spite of the vaccine for the “deadliest virus since the Spanish Flu” allegedly being up to “95% effective in reducing deaths”.
However, although COVID deaths are declining, non-COVID deaths remain at the high end.
So, why is Germany still panicking about COVID and not non-COVID mortality?
Don’t the public health officials actually look at the data?
It’s all here…
Analysis

Looking in more detail at the all-cause mortality data, we can see some peculiar information. Between 2015 and 2020, relative death rates in East and West Germany are distinctly similar (Figure 2). However, since the start of season 2020-21, the East Germans have been dying at an alarmingly higher rate than the West Germans.
Drilling in closer, we can see that the divergence starts after October 2020 (when COVID first starts to make a meaningful impact in Germany).
According to Figure 4, this excess death coincides with COVID deaths, but only on 10th Nov 2020 (to be exact), a month after COVID first starts accounting for excess seasonal mortality1.
Why is COVID killing more East Germans than West Germans from this specific point? More West Germans died in spring 2020 but nowhere near as many more East Germans the following autumn/winter.
Well, according to Google Mobility data (Figure 5), the East Germans did get back to living normally more quickly than the West Germans but that was accompanied by less death in spring 2020 and there really isn’t much between them on 10-Nov-20.
Besides, the spread was consistent in the few weeks before that pivotal date so that wouldn’t account for the sudden change. Moreover, mobility plummets in lockstep in both sides of the country on 11-Dec-20, 11 days before deaths peak. It really doesn’t look like dramatic reductions in mobility are associated with reductions in COVID mortality, does it?
Just in case you were still having doubts about the conclusion, as mobility increases from its low on 28-Dec-20 back to normal levels by the end of May, COVID deaths drop consistently, except for a new distribution that starts somewhere towards the end of Feb ‘21. This point is not associated with any particular change in mobility behaviour.
So, much as we observed in the same analysis of London, restricting the mobility of healthy people does not appear to have any benefit in reducing deaths due to an airborne pathogen. Who knew?
If it’s not mobility differences, what else could account for this disparity between East and West?
According to Figure 6, “full protection” (dose 2) from the “vaccine” did not occur until well into 2021 so that would initially rule that factor out too?
We can again dig deeper, though, just to be sure.

According to Figures 7 and 8, there is some variability in the levels of full (2 doses) and booster (3 doses) “vaccination” rates. Perhaps, if we compare these to COVID cases (average weekly incidence), we can see if higher population levels of vaccination leads to lower cases as some have claimed (albeit not based on any empirical evidence).
Although the vaccination rates are as of Sept ‘22, we can see from the vaccination timeseries of Figure 6 and the cases timeseries of Figure 9 which dose regime we should compare to which period of COVID.
As it happens, I found no statistically significant relationship between COVID cases and vaccines before Aug ‘21.

However, for the period 10-Aug-21 to 11-Jan-22, I did find a negative relationship between cases and boosters. In other words, it appears that regions with higher booster rates had lower incidences of COVID during this period.
Note also that there is a statistically significant relationship between case rates in 2021-22 with 2020-21. In other words, seasonality plays a major role (Figure 11).


Nevertheless, including this relationship in the model accounts for any confounding due to seasonality and other demographic factors, adding weight to the result of the regression analysis.

Looking at the booster coverage map (Figure 12), we can clearly see the regions with the highest booster rates also have the relatively lower incidences. Unfortunately though, since they are all also clustered in the West, perhaps we cannot entirely rule out some spurious correlation between likelihood to be vaccinated given region of residence and the evident seasonality pattern?
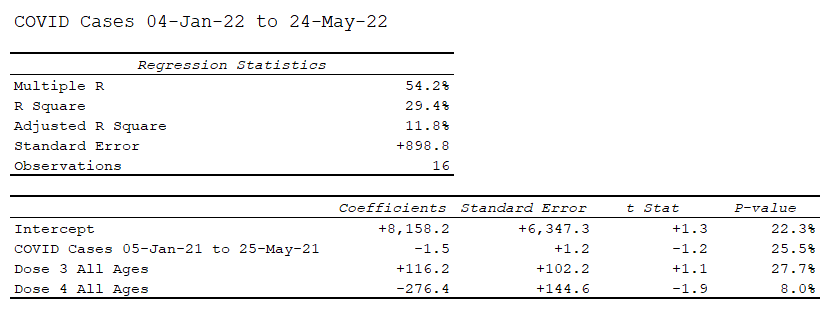
Conversely, looking at the period between 04-Jan-22 and 24-May-22, again controlling using the similar period a year earlier, we can observe no relationship between dose 3 nor dose 4 with COVID incidence.


This time, according to Figure 14, there is no clear seasonal relationship either which further supports the caveat that the prior negative correlation between booster rates and cases may have been spurious.
Moreover, there are ten times as many cases in the more recent period (since the mRNA experiment) than before.

Finally, during the period 31-May-22 to 06-Sep-22, in the absence of any control since there was no COVID in the same period the prior year, we do see a statistically significant relationship with boosters again.
However, this time the coefficient is positive, indicating that the higher booster regions are experiencing the higher incidences of COVID.
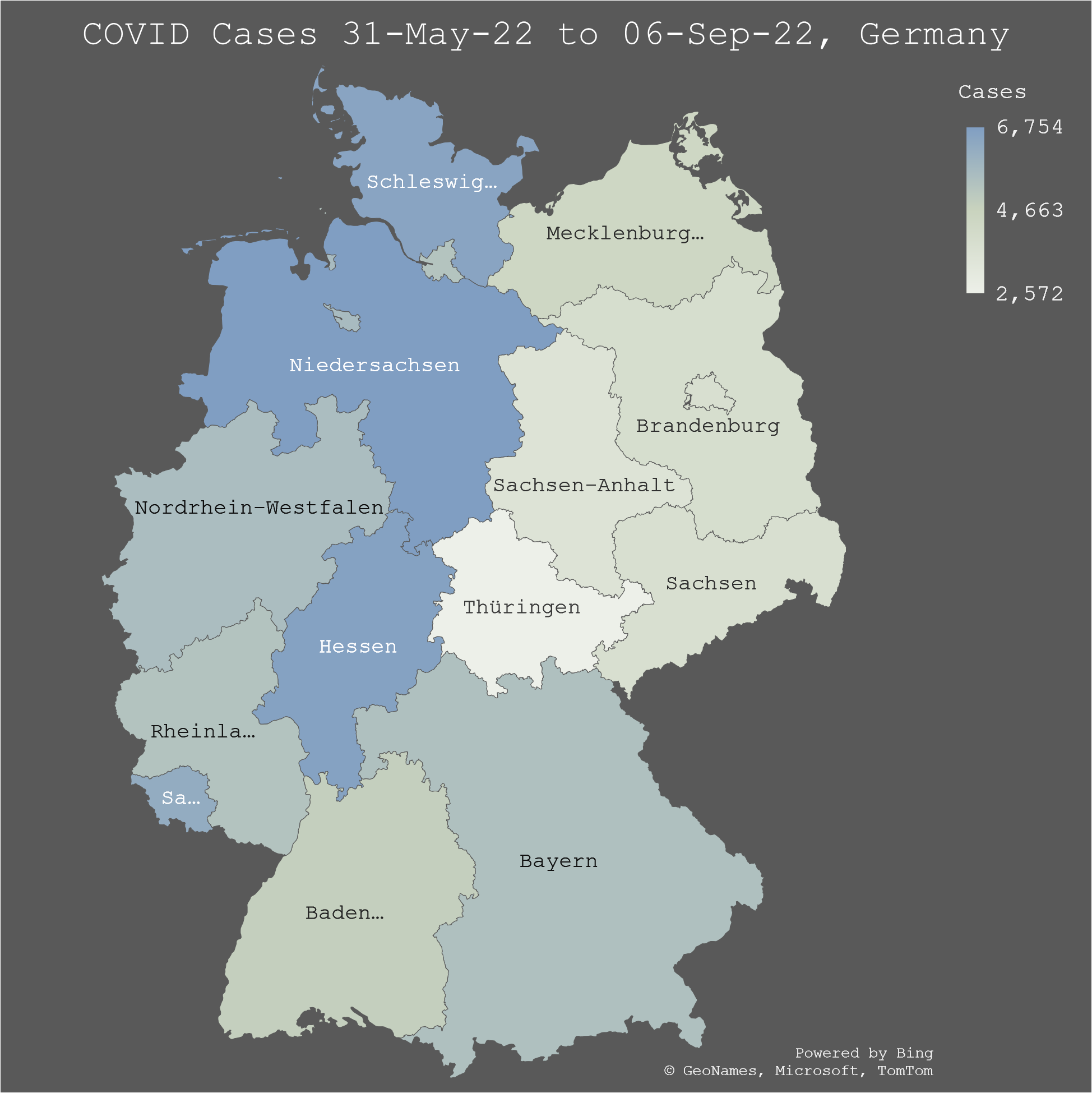
So, to the extent that the apparent benefit of booster rates on COVID incidence is not spurious in Aug ‘21 to Jan ‘22, it is apparently detrimental a few months later. This would, at least, be consistent with the “waning efficacy” hypothesis.
At best then, vaccine efficacy on COVID incidence is inconclusive in my opinion, based on empirical analysis. It is certainly not the strength and quality of evidence that could possibly support the mandating of such an intervention, regardless of other ethical concerns.
If the vaccine is not instrumental in reducing COVID incidence, does it afford any kind of benefit to those at risk of dying from COVID though?
It comes as no surprise (hopefully) to absolutely anyone that COVID presents a substantially higher risk for old people than young. In fact, in 2020, 96% of all COVID deaths in Germany were over 60 years old. So, I’m going to test the over 60s vaccination rates against COVID deaths.
Interestingly, there is a 50% increase in the proportion of COVID deaths aged under 60 from 2021 onwards, after the introduction of the mRNA experiment.

As we can see from Figure 17, more and more younger people succumb to COVID the later we go into the COVID era, whereas the opposite is true for the over 60s (Figure 18). Why is that?
As we have already observed in Figure 7, relatively more older people have been vaccinated than young. Perhaps then, it is the vaccine that is saving them as time goes by and, contrary to the entire history of virology and logic, the virus becomes more virulent?
We can test this hypothesis with some simple regression analysis. There was no vaccination impact on the Wuhan variant COVID of Oct ‘20 to Mar ‘21.

Using the same model as I used for cases, we can see that there is also no correlation between COVID deaths and different vaccination rates across German regions in the period 10-Aug-21 to 11-Jan-22 (Delta variant)(Figure 19).


There is, however, a statistically significant relationship between COVID deaths in this period and the same period a year earlier, before the mRNA experiment started (Figure 20). Seasonality wins again.

There is also no correlation between vaccination rates and COVID deaths during the period 04-Jan-22 and 24-May-22 (Omicron BA.1 variant)(Figure 21).


The relationship with the prior season is not significant even though there does appear to be some seasonality looking at the map (Figure 22).
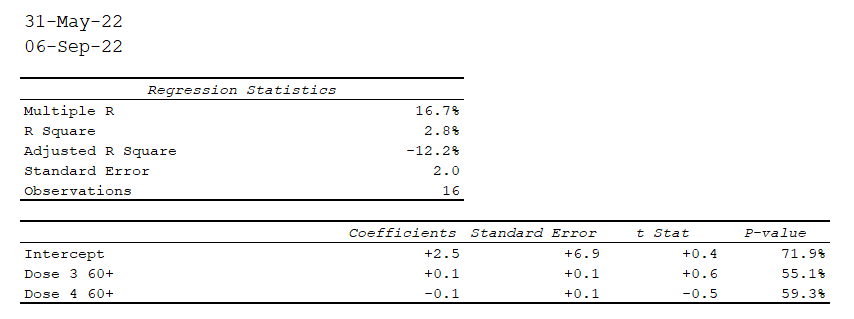
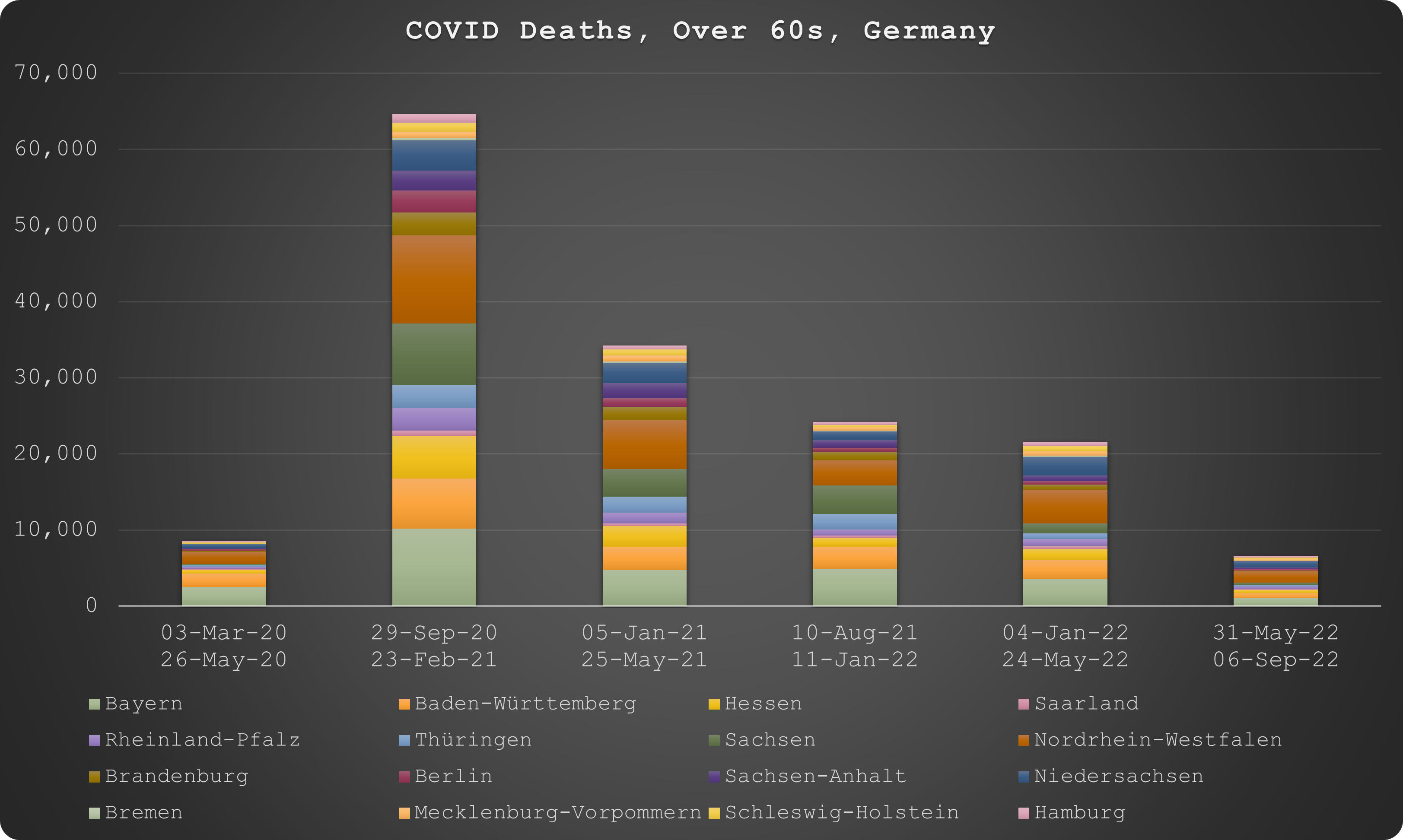
Finally, there is no correlation between COVID deaths and vaccination rates for the period 31-May-22 to 06-Sep-22, for which there is no reference period the prior year given how unusual it is for a seasonal virus to have an impact in the middle of summer (Figures 23 and 24).

In spite of the unseasonal deaths, overall there are fewer weekly deaths the further into the COVID era we progress. This is to be expected for a virus whose natural selection should be the variant that is most transmissible and least virulent.
In one final analysis, we should also consider healthcare disparity. To analyse this, we can look at the relative case fatality rates (CFRs) between East and West Germany.
According to Figure 25, the CFRs appear reasonably comparable. However, at the peak in Dec ‘20, the CFR for East Germany is more than 1% higher than West Germany.
In fact, across the whole month the CFR increase ranges between 0.7% and 1.1% vs an average incidence of almost 16,000 cases per million population each week for East Germany and 14,000 for West Germany. Mathematically, this would produce an increase of roughly 150 deaths per million per week.
Conclusion
While I cannot conclusively explain why more East Germans have died in association with COVID than West Germans, I can confidently conclude that it is not as a result of different behaviour or different vaccination rates.
Nevertheless, there must be something particular that accounts for this disparity and it manifests predominantly since mid-Nov 2020.
The case fatality rate for East Germans is almost 20% higher during the peak mortality periods and it appears that East Germany also suffers higher incidence of virus too.
So, it seems to me that a combination of poorer health and/or healthcare, and poorer climate are most likely to be the reason why COVID was worse for the East than the West.
The German data reports COVID death on date that the deceased tested positive, not on the date of death. This means the data will not correlate exactly with all-cause deaths (due to the typical 3 to 4 week period between infection and death) but does make it easier to measure the impact of COVID interventions on COVID deaths.
Consider Mathew Crawford's theory of "wealth effect." Isn't East Germany significantly less wealthy?
I think the higher mortality of East is caused by collapse of hospital care. Basically, many hospitals in East were under financed for long time and combined with overload caused by the new covid measures and first lockdown, it totally breaks hospital care. The same is for the hospital staff, some of the nurses and doctors were just too scared by this covid propaganda, so they stayed home or returned to their home country and even reduce the already low hospital capacity further.
The more I see this kind of analyses, the more I know that it was not the virus but the restrictions and issue of money or wealth. Normal viruses didn't distinguish between rich and poor, but this covid does.