


Did Hungary's preference for Sinopharm (China) and Sputnik (Russia) COVID "vaccines" avoid thousands of deaths?
Analysis of European excess mortality reveals a number of startling anomalies.

Voiceover provided by audyo.ai or listen in the standalone audyo player:

Introduction
I have shown in previous analyses that there appears to be a “longitudinal” relationship amongst European countries when analysing all-cause mortality throughout the entire year.
Although, there is no plausible explanation for this in terms of physical geography, I have surmised that perhaps there is some element of human geography, demographics or some other socioeconomic factors that might explain this.
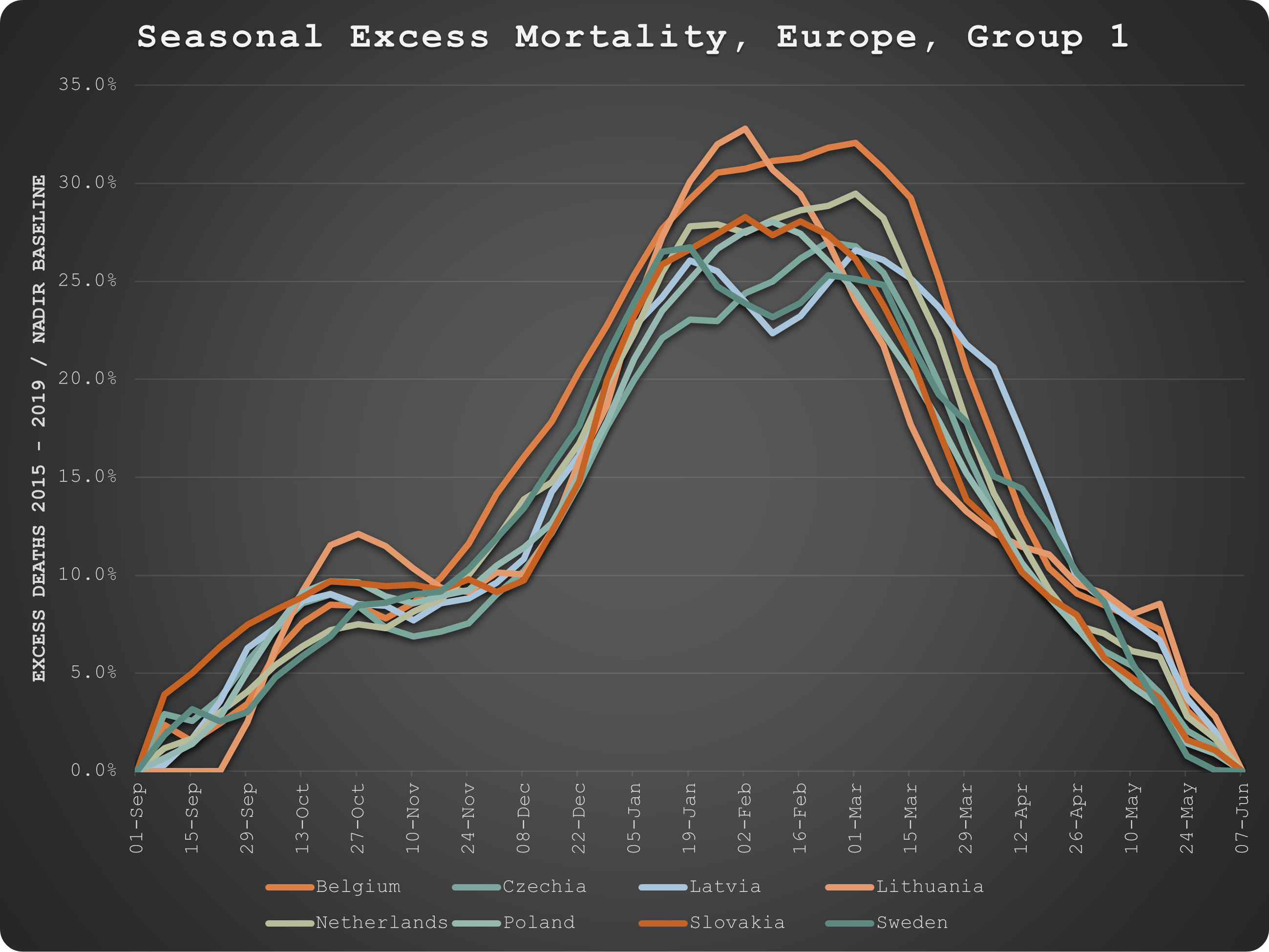
In this analysis, I model seasonal excess mortality and the results fall logically into latitudinal groupings that would be consistent with various hypotheses of “winter” respiratory pathogens contributing to seasonal excess deaths.
In fact, in a “Hope-Simpson” moment, I discovered three main types of mortality distribution:


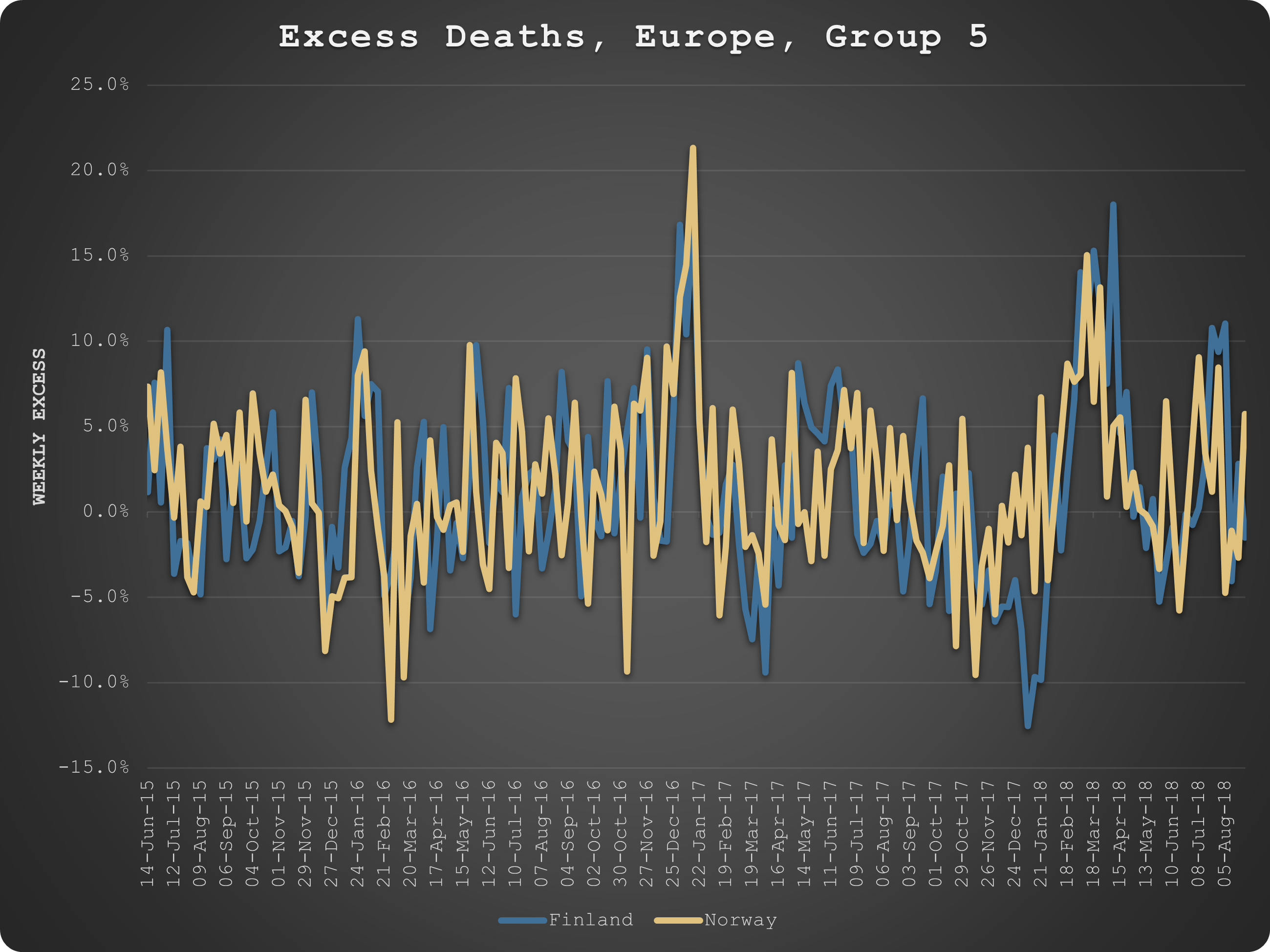
Four countries did not fit into the three main groups:


When we look at these groupings on a map, the result should satisfy even the most narrow-minded physical geographer:

Pre-COVID Seasonal Variation in Excess Death
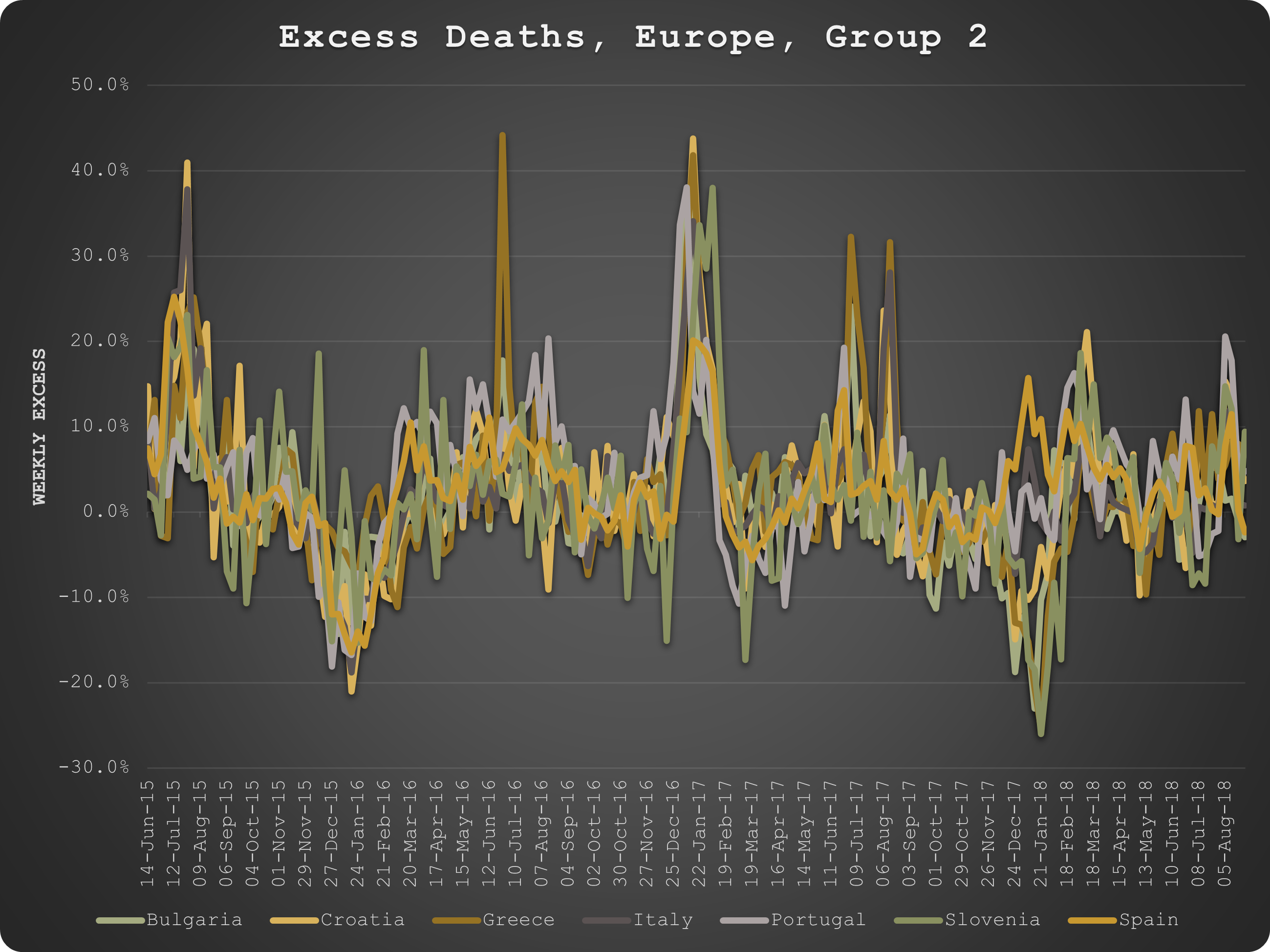
Historically, when there has been an unusually harsh1 or soft “season”, the effects are synchronous within the identified groups, both in terms of timing and relative magnitude, as we should expect.



Logically then, if we accept the premise that COVID disease results from SARS-CoV-2 which is a respiratory pathogen then we should expect to see similar mortality patterns within these groups, shouldn’t we?
But we don’t.
COVID Deaths
The timings and relative magnitude of COVID mortality do not follow the expected patterns dictated by historical, seasonal patterns.





COVID hits same group countries at different times and magnitudes, even completely different seasons.
This did not make sense to me so I reorganised the countries by COVID death distribution2 and once again, we have a similar pattern to the original analysis, suggesting once again that something else (i.e. not a "typical" respiratory pathogen) is primarily responsible for COVID-labelled (excess) deaths.

The Fragile Healthcare Hypothesis
I reconsidered the fragile healthcare hypothesis to explain these unexpected results.
Even though all countries enacted the same ludicrous and futile measures to “control” the spread of the virus, thereby causing massive disruption to fragile health and social welfare systems, only Western European countries suffered in spring 2020 because COVID did not emerge in the East until the following autumn.
When it did, it was even more impactful - perhaps because those poorer nations were even worse equipped to deal with the disruption on top of the fact that COVID emerges at the start of the mortality season rather than the end?
Whilst this hypothesis is appealing, it does not address the question as to why there was no COVID at all in the East during the initial epidemic.
As we have seen in many other studies, this is unlikely to be due to the “success” of transmission mitigation strategies. Furthermore, it would not explain why this respiratory pathogen appears to emerge in the west and spread eastwards?
So, I’m still left to consider a complementary hypothesis to explain this critical fact. Fear not, I am working on it, having recently been invited to a working group of scientists who specialise in the deleterious effects of various types of radiation. So, hold onto your tin foil hats!!

The Wealth Factor
Another undeniable fact is the relationship between wealth and COVID mortality. A logarithmic regression of normalised COVID deaths and GDP per capita has an R-squared of almost 80%.
Sure enough, there is a strong relationship between COVID deaths and excess deaths too.
Again, this is logical, as one would expect wealthier countries to have better healthcare facilities to treat sick people and perhaps even better metabolic health as well. Doesn’t that make you wonder why any country would completely disregard the potential economic cost of nationwide measures to “control the spread”?
This, again, belies the premise that outcomes are positively affected by transmission mitigation strategies. The outcomes are a function of treatment. If focus had been on treatment of sick people instead of curtailment of activity of healthy ones, who knows how many more lives could have genuinely been saved?
But, now here’s where it gets really interesting...
Although the relationship between COVID deaths and excess deaths is strong (see above), when we look at the patterns, we observe that for some countries, there are more COVID deaths than excess deaths, for others there are exactly the same and for others, there are more excess deaths than COVID deaths.

As it happens, the countries with less excess deaths than COVID deaths, are pretty much the wealthy ones again! Moreover, the disparity starts after the initial shock to the system in the presence of the disease.
Take Belgium, for example but they are all very similar:

This lends further support to the the premise of the fragile healthcare hypothesis. Those wealthier countries have not suffered hardly any excess death since they lifted the disruption to their systems.
However, if we accept this hypothesis, it seems that the poorer countries are yet to fully recover, like Croatia, for example:

And then there are countries like Lithuania whose policies are simply killing its citizens regardless of the presence of COVID or not!

The “Vaccine” Dilemma
Since COVID deaths have pretty much continued unabated across the whole of Europe “in spite” of the “life-saving” “vaccine”, there is little support for the premise that it is effective.
But is there evidence that it actually does harm?
I have another hypothesis that the reason why the poorer countries have experienced so much more excess death (and COVID death) than their richer western neighbours since the start of the mass experiment is once again due to quality of healthcare. I surmise that they are simply not equipped to deal with the deluge of injuries caused by the vaccination programs.
I was confident of this hypothesis until I tabled the data (above) and noticed Hungary sticking out like a sore thumb. How on earth has Hungary suffered so little excess death relative to its peer groups in this analysis? It really should be more like Bulgaria, Lithuania, Romania and Slovakia when everything is taken into account?
Anyway, I did a little digging around and discovered one unique but rather important fact about Hungary - they are the only European country to have administered China’s Sinopharm vaccine (inactivated whole virus) and Russia’s Sputnik vaccine (non-replicating viral vector like Astra Zeneca) in preference to Pfizer and Moderna’s RNA products.
In fact, almost half of Hungary’s vaccination program is not RNA product, compared to 85%+ that is for the rest of Europe. Conversely, Lithuania which has the worst excess death to COVID death ratio and the second worst excess death overall is the only country with virtually 100% RNA product administration.

I wonder, could that be an important fact? Or just another conspiracy theory?
Measured as “super” excess, i.e. excess over the seasonal excess which in turn was a function of the “nadir” baseline.
Note: Neither Greece nor Portugal resembled any other country so they have been omitted.
Great post and excellent work!
We will probably never know what was in the China and Russia jabs. They may have been mostly placebo. There appears to be a democide going on in the western countries.